Introduction
- Radiofrequency ablation (RFA) is a minimally invasive thermal ablation technique to treat benign thyroid nodules causing compressive or cosmetic complaints (figure 1).
- The American Thyroid Association statement on thyroid nodule ablation techniques considers cytologically indeterminate thyroid nodules (ITNs) with negative molecular markers to be a relative contra-indication for RFA.1
- The Afirma Genomic Sequencing Classifier (GSC) benign molecular result in thyroid nodules with Bethesda (B) III or IV cytology has a risk of malignancy similar to a Bethesda II cytology result.2,3
Study Aim
The objective of this study is to analyze the efficacy of RFA in ITNs with a benign Afirma GSC molecular result.
Methods
- This is a retrospective, multicenter, cohort study of 18 patients who underwent RFA between January 2021 and December 2022 with ITN (BIII or IV) and benign Afirma GSC testing.
- Clinical data was collected under WCG IRB protocol DHF 005-077.
- A historical cohort with cytologically benign nodules was compared and the volume reduction percentage (VRP) was assessed. A paired t-test compared the pre- and post RFA changes.
Results
- Eighteen (16 Bethesda III and 2 Bethesda IV) study nodules (15 females, 3 males: median age 42 [interquartile range (IQR) 38-49]) were analyzed (table 1).
- Median follow up was 123 days [IQR 67-356].
- Thirteen samples were non-functional thyroid nodules (NFTN) and 5 were autonomously functioning thyroid nodules (AFTN).
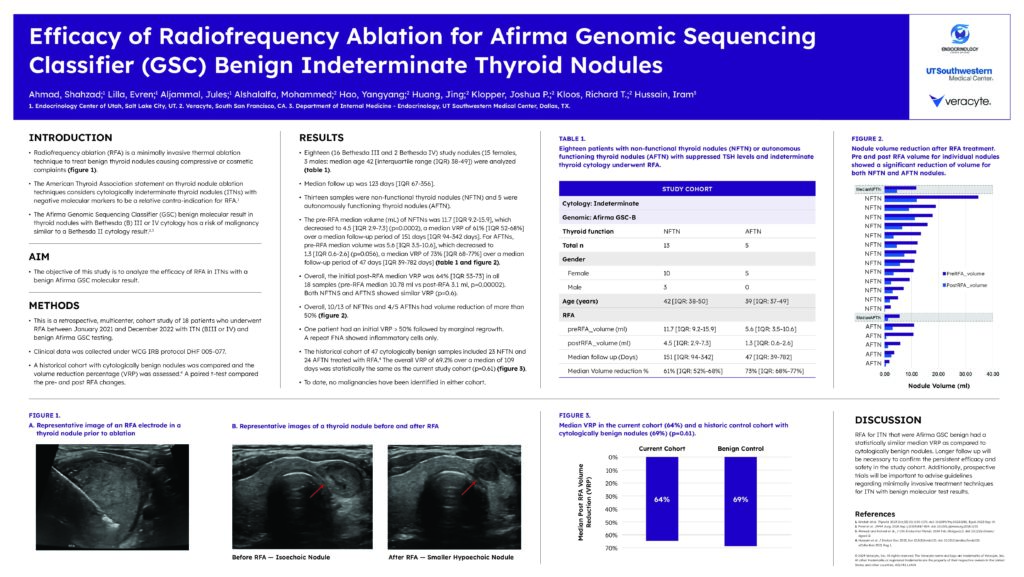
- The pre-RFA median volume (mL) of NFTNs was 11.7 [IQR 9.2-15.9], which decreased to 4.5 [IQR 2.9-7.3] (p=0.0002), a median VRP of 61% [IQR 52-68%] over a median follow-up period of 151 days [IQR 94-342 days]. For AFTNs, pre-RFA median volume was 5.6 [IQR 3.5-10.6], which decreased to 1.3 [IQR 0.6-2.6] (p=0.056), a median VRP of 73% [IQR 68-77%] over a median follow-up period of 47 days [IQR 39-782 days] (table 1 and figure 2).
- Overall, the initial post-RFA median VRP was 64% [IQR 53-73] in all 18 samples (pre-RFA median 10.78 ml vs post-RFA 3.1 ml, p=0.00002). Both NFTNS and AFTNS showed similar VRP (p=0.6).
- Overall, 10/13 of NFTNs and 4/5 AFTNs had volume reduction of more than 50% (figure 2).
- One patient had an initial VRP > 50% followed by marginal regrowth.
- A repeat FNA showed inflammatory cells only.
- The historical cohort of 47 cytologically benign samples included 23 NFTN and 24 AFTN treated with RFA.4 The overall VRP of 69.2% over a median of 109 days was statistically the same as the current study cohort (p=0.61) (figure 3).
- To date, no malignancies have been identified in either cohort.
Conclusion
RFA for ITN that were Afirma GSC benign had a statistically similar median VRP as compared to cytologically benign nodules. Longer follow up will be necessary to confirm the persistent efficacy and safety in the study cohort. Additionally, prospective trials will be important to advise guidelines regarding minimally invasive treatment techniques for ITN with benign molecular test results.
Conference Materials
Afirma Thyroid
Efficacy of Radiofrequency Ablation for Afirma Genomic Sequencing Classifier (GSC) Benign Indeterminate Thyroid Nodules
Ahmad S, et al. AACE. 2024. DOI: 10.1016/j.eprac.2024.03.058.