Afirma GSC Shows Value in Ruling Out Malignancy in Indeterminate Thyroid Nodules (ITN)
An indeterminate thyroid nodule (ITN) carries a ~25% risk of malignancy (ROM), and historically diagnostic surgery for ITNs revealed a benign histopathology in 75% of cases.1
Molecular testing attempts to help prevent unnecessary surgeries with a focus on “rule-out” metrics such as Sensitivity (SN) and Negative Predictive Value (NPV). Tests may be optimized to keep the false negative rate low in validation studies, but how does that translate into real-world outcomes?
Ahmadi et al. sought to evaluate the performance of Afirma GSC’s rule-out capabilities in their evaluation of over 800 Bethesda III/IV nodules, with a median follow-up time of 23 months.
In this independent, multicenter study, the authors sought to understand key performance metrics, including SN and NPV in their evaluation of real-world patient outcomes.
Afirma GSC Demonstrated Strong Performance in Line with Validation Study Metrics
When stratifying performance metrics between Bethesda III and Bethesda IV nodules, Afirma GSC performed similarly across these two nodule types. While some studies may have a limited number of higher-risk Bethesda IV nodules included in the cohort,2 a total of 215 Bethesda IV nodules were evaluated by Ahmadi et al. Notably, the SN and NPV performance were in line with or above the validation study.3
Given that 80% of patients with Bethesda IV cytology who do not undergo molecular testing end up having surgery,4 Afirma GSC can confidently identify benign nodules in Bethesda IV cytology to help prevent unnecessary surgeries for these patients.
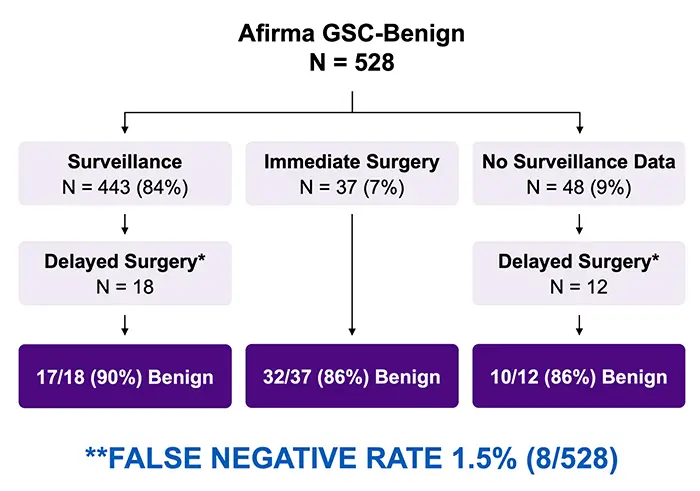
Ahmadi et al. Found That Afirma Demonstrated a False Negative Rate of 1.5%
When looking at performance among Afirma GSC Benign nodules, 528 patients received an Afirma GSC Benign result for a Benign Call Rate (BCR) of 63% overall. With the majority undergoing surveillance (N = 443) and some patients opting for surgery – including delayed surgery – the overall false negative rate is 1.5% (8/528 nodules) when assuming the unoperated Afirma GSC Benign nodules would have been benign had they been removed.
Clinical Management of Afirma GSC Benign Nodules
Ultimately, Ahmadi et al. found that Afirma GSC can be a key tool for managing patients with indeterminate cytology in a variety of practice settings and prevalence of malignancy. The majority of GSC-benign nodules remained stable over the surveillance period, and the authors found that “GSC-benign thyroid nodules can be observed similarly to thyroid nodules with benign cytology”,5 reinforcing Afirma’s “rule-out” capabilities.