May is Bladder Cancer Awareness Month—a meaningful time to spotlight a disease that will be diagnosed in nearly 85,000 people in the U.S. this year alone and is expected to claim more than 17,000 lives, according to the American Cancer Society.1
Unfortunately, the bladder cancer patient journey is rarely straightforward. From vague initial symptoms to high rates of disease recurrence and challenging treatment decisions, patients and clinicians alike often face uncertainty at nearly every stage.
Fortunately, advances in genomic technology now offer new tools to help clinicians and their patients make better-informed and more-confident treatment decisions based on the biology of each patient’s cancer.
Understanding Bladder Cancer
Bladder cancer most commonly affects older adults, with 90% of cases2 occurring in people over age 55 and the average age at diagnosis being 73. Smoking is the most common risk factor. While bladder cancer’s symptoms—such as blood in the urine, increased urination frequency or urgency, or pain during urination—can be mistaken for other conditions, early diagnosis is important.
Diagnosis of bladder cancer typically involves cystoscopy, in which a camera is used to visualize the inside of the bladder. If cancer is suspected, generally patients are offered a transurethral resection of a bladder tumor (TURBT), a procedure that is both diagnostic and therapeutic. Once definitively diagnosed, patients are categorized as having:
- Non-muscle-invasive bladder cancer (NMIBC) – where cancer is confined to the inner lining of the bladder (about 70% of cases3); or
- Muscle-invasive bladder cancer (MIBC) – where cancer has penetrated the muscle wall or beyond (about 30% of cases).
MIBC is considered more aggressive and requires urgent intervention. However, both NMIBC and MIBC have high rates of recurrence, with the cancer typically requiring lifelong follow-up care.
Navigating a Complex Treatment Journey
Treatment of NMIBC and MIBC differ significantly and each typically involves multiple steps.
- NMIBC treatment often includes intravesical therapy, in which a liquid drug – typically the immunotherapy Bacillus Calmette-Guerin (BCG) or a chemotherapy cocktail (gemcitabine and docetaxel) – is delivered directly into the bladder. If patients respond well to intravesical therapy, they will typically receive maintenance treatment for 1-3 years. If they do not respond well to intravesical therapy, clinical guidelines recommend radical cystectomy (RC) or chemotherapy plus radiation; other options include RC, systemic chemotherapy, immunotherapy, or intravesical investigational drugs.
- MIBC treatment typically involves neoadjuvant chemotherapy (NAC) followed by radical cystectomy or a combination of systemic chemotherapy and radiation. In some cases, additional chemotherapy or immunotherapy may be administered after surgery or radiation.
Treatment decisions to date have been primarily guided by the cancer’s grade and stage, which are informed by histopathology and imaging scans. These clinical risk factors, however, can be imprecise, which can lead to patients being overtreated or undertreated. In fact, data show that approximately 40% of patients with NMIBC are upstaged at radical cystectomy4 to MIBC. The growing number of treatment options available further adds to the complexity.
Genomic Technology as a Better Guide
This is where advanced genomic technology comes in.
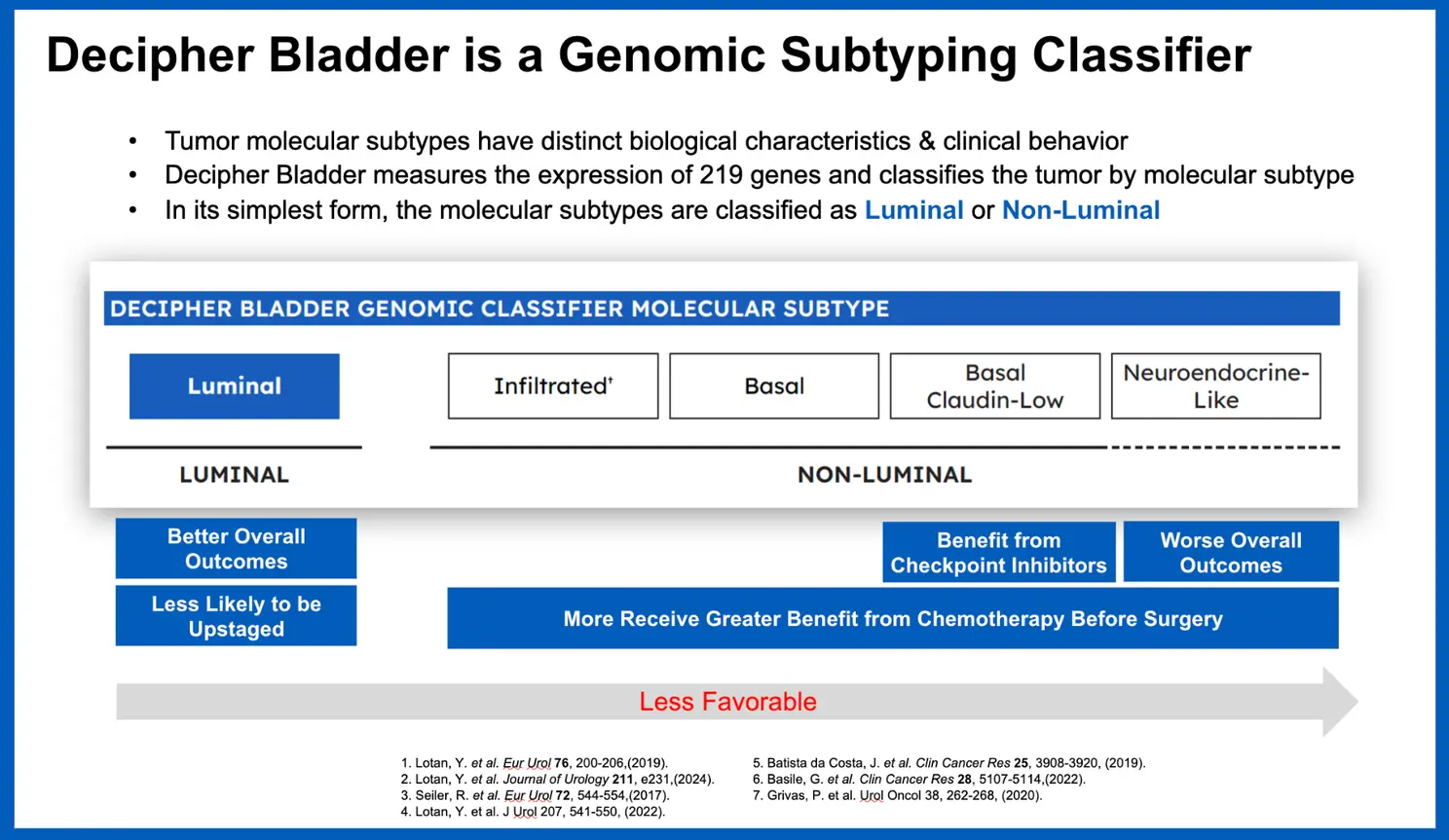
The Decipher Bladder Genomic Subtyping Classifier is a clinically available genomic test that provides a deep biological characterization of each patient’s bladder tumor to help guide treatment decisions for patients with NMIBC or MIBC. Developed through RNA whole-transcriptome analysis and machine learning, the 219-gene test classifies bladder tumors into five distinct molecular subtypes—each with unique biology and potential treatment implications. This information can help guide decisions at key moments in a patient’s care journey.
Building Rigorous Clinical Evidence
The Decipher Bladder test is supported by a dozen published studies demonstrating its performance and clinical utility. Such clinical evidence has led to the test’s coverage by Medicare and growing interest among clinicians.
Just recently, a study published in European Urology Open Science showed that the test can identify patients whose disease may be more aggressive than initially staged via TURBT.
Additionally, through its whole-transcriptome-based Decipher GRID (Genomic Resource for Intelligent Discovery) research tool, Veracyte and its collaborators are deriving additional insights that may ultimately impact patient care. For example, among nearly 20 abstracts presented on our Decipher Prostate and Bladder tests at the recent American Urological Association annual meeting, researchers used Decipher Bladder GRID to identify a subset of patients with high-risk NMIBC who responded better to therapy with sequential intravesical gemcitabine and docetaxel (Gem/Doce), compared to guideline-recommended intravesical Bacillus Calmette-Guerin (BCG), based on their tumors’ underlying biology. Such findings could be particularly helpful, given ongoing supply challenges with BCG.
What’s Next: Bladder Cancer MRD Testing
After completing curative treatment—such as surgery, chemotherapy, or radiation—clinicians and patients are often left with lingering questions such as: Has the cancer truly been eliminated? Is more treatment needed? Traditional imaging and pathology often can’t detect small amounts of residual disease, which can lead to over-, under- or delayed treatment —all of which can negatively impact patient outcomes.
To address this, Veracyte is developing a novel minimal residual disease (MRD) test for MIBC, which is performed on a patient’s blood sample following treatment. The test uses a combination of whole-genome sequencing and artificial intelligence (AI) to enable earlier detection and improved outcomes throughout the patient’s treatment and follow-up care.
In a podium presentation at the recent European Association of Urology Congress (EAU25), investigators shared promising findings from the large, independent, interventional TOMBOLA trial, which showed that Veracyte’s MRD testing platform detected cancer in patients treated for MIBC with more accuracy than digital droplet PCR and approximately three months earlier than standard imaging techniques.
At every stage of the bladder cancer journey, clinicians and patients face difficult decisions—often with limited information. Genomic advances like the Decipher Bladder test are helping to change that by delivering meaningful biological insights that can lead to more personalized, informed, and effective care. Because better insights lead to better outcomes.